News & Events
TSH receptor autoantibody secrets you should know now
Sep
Have you ever wondered why you feel tired, anxious, or notice changes in your weight without a clear reason? You might have a thyroid problem, and you are not alone.
- About 10% of people in the United States have thyroid antibodies.
- Graves’ disease, which features stimulating TSH receptor autoantibodies, affects 2–3% of the population.
| Why It Matters Now | What You Gain |
|---|---|
| TSH receptor autoantibodies play a key role in thyroid disorders like Graves’ disease. | Understanding these antibodies helps you recognize symptoms, seek the right tests, and make informed choices about your health. |
You need to know how tsh receptor autoantibody testing can reveal hidden causes of your symptoms. With simple facts, you will learn what makes tsh receptor autoantibodies so important right now.
Key Takeaways
- TSH receptor autoantibodies are crucial for understanding thyroid health. They help identify conditions like Graves’ disease, which affects 2-3% of the population.
- Testing for TSH receptor autoantibodies can reveal hidden thyroid issues. If you experience symptoms like weight changes or a fast heartbeat, ask your doctor about testing.
- There are three types of TSH receptor autoantibodies: stimulating, blocking, and neutral. Each type affects thyroid function differently, influencing your symptoms and treatment.
- High levels of TSH receptor autoantibodies often indicate Graves’ disease. Monitoring these levels helps doctors tailor treatment and predict potential complications.
- Stay informed about your thyroid health. Regular checkups and open communication with your doctor empower you to manage your condition effectively.
TSH Receptor Autoantibody Basics

What Are TSH Receptor Autoantibodies?
You may wonder what makes your thyroid act up. TSH receptor autoantibodies are special proteins your immune system can make by mistake. These proteins target the thyrotropin receptor, which sits on the surface of your thyroid cells. Normally, the thyrotropin receptor responds to thyroid stimulating hormone and helps control how much thyroid hormones your body makes. When these autoantibodies bind to the receptor, they can change how your thyroid works. Scientists have found that these autoantibodies play a big role in autoimmune thyroid disease, especially in Graves’ disease. New tests can now find these autoantibodies more accurately, but sometimes the tests cannot tell if the antibodies are helping or hurting the thyroid.
Note: TSH receptor autoantibodies are different from other thyroid antibodies, like anti-TPO or anti-thyroglobulin antibodies. Anti-tsh receptor antibodies show up in most people with Graves’ disease, but not as often in other thyroid problems.
Types: Stimulating, Blocking, Neutral
Not all TSH receptor autoantibodies act the same way. You can think of them as three main types, each with a different job:
| Type of Antibody | Function | Effect |
|---|---|---|
| TSH-R-stimulating Ab (TSAb) | Activates thyrotropin receptor | Causes hyperthyroidism in Graves’ disease |
| TSH-R-blocking Ab | Blocks TSH action | Can lead to hypothyroidism in autoimmune thyroid disease |
| Neutral Ab | No clear effect | May have unknown or subtle effects on thyroid cells |
Stimulating antibodies turn the thyrotropin receptor “on,” making your thyroid produce too much hormone. Blocking antibodies do the opposite and can slow down your thyroid. Neutral antibodies do not seem to change thyroid function, but researchers still study them to learn more.
How They Affect the Thyroid
TSH receptor autoantibodies can change how your thyroid works in several ways:
- These autoantibodies can act like a switch. Stimulating antibodies flip the switch “on,” causing your thyroid to make too much hormone. This leads to hyperthyroidism, which is common in Graves’ disease.
- Blocking antibodies flip the switch “off,” which can slow down hormone production and cause symptoms of low thyroid.
- Sometimes, both types of antibodies show up together. This can make it hard for doctors to figure out what is happening in your body.
When stimulating antibodies bind to the thyrotropin receptor, they mimic the action of thyroid stimulating hormone. This makes your thyroid cells work overtime and release extra thyroid hormones. You may feel nervous, lose weight, or have a fast heartbeat. In Graves’ disease, almost all patients have these stimulating antibodies. Studies show that most people with Graves’ disease have active antibodies that bind to the thyrotropin receptor, while people without the disease do not.
Tip: Doctors use special tests to look for these autoantibodies. High levels often mean you have Graves’ disease, but the type of antibody matters for your symptoms and treatment.
You should know that these autoantibodies are not the same as other thyroid antibodies. Anti-tsh receptor antibodies are found in most people with Graves’ disease, but anti-TPO antibodies are more common in other autoimmune thyroid diseases.
Graves’ Disease and TSH Receptor Autoantibodies
Pathogenic Role in Graves’ Disease
You may hear doctors call stimulating TSH receptor autoantibodies the “hallmark” of Graves’ disease. These antibodies target the thyrotropin receptor on your thyroid cells. When they bind to the receptor, they do not just mimic normal hormone signals. They actually push your thyroid cells to grow and survive longer than they should. This happens because the antibodies activate important cell pathways, like PKA/CREB and AKT/mTOR/S6K. These pathways tell your thyroid to keep working and growing. As a result, your thyroid gland becomes overactive. This overactivity is what sets Graves’ disease apart from other types of autoimmune thyroid disease.
You should know that most people with Graves’ disease have these antibodies. Studies show that:
- TSH-binding inhibiting antibodies appear in about 68.8% of people with Graves’ disease.
- Thyroid stimulating antibodies show up in about 77.8% of people with Graves’ disease.
Doctors often use these numbers to help confirm a diagnosis. If you have symptoms and test positive for anti-tsh receptor antibodies, you likely have Graves’ disease.
The persistence of anti-tsh receptor antibodies can affect your thyroid health for years. Some people may shift between different types of antibodies, which can change how their thyroid works over time.
Hyperthyroidism and Antibody Action
When you have Graves’ disease, your body makes TSH receptor autoantibody that stimulates the thyrotropin receptor. This causes your thyroid to release too much hormone. You may notice signs of hyperthyroidism, such as:
- Fast heartbeat or palpitations
- Feeling hot or sweating more than usual
- Shaky hands or tremors
- Eyes that seem to stare or have lid lag
- Needing to use the bathroom more often
- Losing weight even though you eat more
- Weakness in your upper arms or legs
- Feeling anxious or even having mood changes
If you do not treat hyperthyroidism, you may develop serious heart problems. Some people get atrial fibrillation, which is a fast and irregular heartbeat. Others may develop heart failure. These problems can happen in up to 15% of people with untreated Graves’ disease.
TSH receptor autoantibody does not only affect your thyroid. You may also see changes outside your thyroid. Doctors call these extrathyroidal symptoms. The most common are:
- Graves’ orbitopathy (eye problems)
- Graves’ dermopathy (skin changes)
- Acropachy (swelling of fingers and toes)
These symptoms happen because the same thyrotropin receptor appears in other tissues, not just your thyroid.
Pediatric Graves’ Disease
Children can also develop Graves’ disease, but it is less common than in adults. About 1 in 10,000 children get this condition. Graves’ disease causes more than 95% of hyperthyroidism cases in children. If your child has symptoms like weight loss, fast heartbeat, or mood swings, doctors may check for anti-tsh receptor antibodies.
| Aspect | Detail |
|---|---|
| Prevalence of Graves’ disease | Approximately 1 in 10,000 in pediatric populations |
| Contribution to hyperthyroidism | Accounts for more than 95% of childhood cases of hyperthyroidism |
Some children have other health conditions, like type 1 diabetes. In these children, doctors often find lower levels of TSH receptor autoantibody at diagnosis. They may also have fewer symptoms and lower thyroid hormone levels. For example:
- About 2.3% of children with type 1 diabetes also have Graves’ disease.
- These children usually have milder symptoms.
- They also show lower free T4 and TSH receptor autoantibody levels when diagnosed.
If your child has type 1 diabetes, you should watch for signs of thyroid problems. Early testing can help doctors manage both conditions better.
Detection of TSH Receptor Autoantibodies

Laboratory Tests
You can find out if you have TSH receptor autoantibodies with a simple blood test. The most common test is the TRAb test. This test measures antibodies that target the thyrotropin receptor on your thyroid cells. The TRAb test uses electrochemiluminescence to detect these antibodies. Doctors often order this test if you have symptoms of hyperthyroidism, such as weight loss, rapid heartbeat, or eye changes.
| Test Name | Description | Mechanism |
|---|---|---|
| TRAb Test | Measures TSH receptor autoantibodies | Uses electrochemiluminescence detection to identify antibodies binding to TSH receptor, affecting thyroid function. |
You may also hear about the IMMULITE TSI assay. This test has a sensitivity of 98.6% and a specificity of 96.4%. These numbers mean the test can find most people with Graves’ disease and rarely gives a false positive.
- The TRAb test detects autoantibodies linked to hyperthyroidism and Graves’ disease.
- High results can confirm Graves’ disease or help tell it apart from other thyroid problems.
Understanding Results
When you get your test results, you want to know what they mean. High levels of TSH receptor autoantibodies usually point to Graves’ disease. Doctors look at the amount, or titer, of these antibodies. High titers are strong markers for Graves’ disease and its complications, like Graves’ orbitopathy. The presence of these antibodies also helps doctors see how severe your disease is.
| Aspect | Details |
|---|---|
| TSH-R-Abs Role | May mimic or block thyroid stimulating hormone action or be neutral. |
| Specificity | Stimulating TSH-R-Abs are specific biomarkers for Graves’ disease. |
| Diagnostic Utility | Used for rapid diagnosis and to tell Graves’ disease from other autoimmune thyroid disease. |
Doctors use these results to guide your treatment. If your antibody levels stay high, you may need closer follow-up.
Tip: High titers of anti-tsh receptor antibodies can mean a higher risk of complications, especially if you have eye symptoms.
When to Test
You should get tested if you have signs of hyperthyroidism or if your doctor suspects an autoimmune thyroid disease. The TRAb test is best for people with new symptoms or when doctors need to confirm Graves’ disease. You do not need both TRAb and TSI tests at the same time, as one is enough.
| Clinical Scenario | Recommendation |
|---|---|
| Hyperthyroidism | Use a single TSH receptor antibody test (TRAb) to assess autoimmune-mediated hyperthyroidism. |
| Autoimmune Thyroid Diseases | Consider TRAb testing for diagnosis and to avoid extra costs. |
Doctors may also test you if you have thyroid eye disease or if you need to know the cause of your thyroid hormone changes. Testing helps you and your doctor make the best plan for your health.
Anti-TSH Receptor Antibodies in Diagnosis & Treatment
Diagnostic Value
You can rely on anti-TSH receptor antibodies for both diagnosis and management of thyroid disorders. These antibodies help your doctor tell the difference between graves’ disease and other causes of hyperthyroidism. Sensitive assays of anti-tsh receptor antibodies, like TRAb and TSI, show high accuracy.
- TRAb tests reach a sensitivity of 96.6% and specificity of 97.1%.
- TSI tests show a sensitivity of 98.8% and specificity of 96.4%.
- When doctors compare graves’ disease to other types of hyperthyroidism, TRAb tests still perform well, with a sensitivity of 92.0% and specificity of 89.1%.
You see the clinical utility of tsh receptor antibodies in these numbers. They help confirm graves’ disease and guide your next steps.
Monitoring and Prognosis
Doctors use anti-TSH receptor antibody levels to track your disease and predict what may happen next. Higher levels often mean more severe symptoms, especially with eye problems or swelling. The table below shows how different tests relate to disease severity:
| Assay Type | Correlation with CAS (β) | Correlation with Proptosis (β) |
|---|---|---|
| TRAb1st | 0.21 | 0.38 |
| TRAb3rd | 0.21 | 0.34 |
| Mc4-CHO TSI | 0.46 | 0.33 |
Doctors notice that if your antibody levels stay high after treatment, you may not respond well. A smaller drop in these antibodies after therapy can mean a higher risk of poor outcomes. You should know that high levels before treatment often predict high levels after treatment.
You can also use antibody tests to predict relapse or remission. The chart below shows how well different tests predict relapse in graves’ disease:
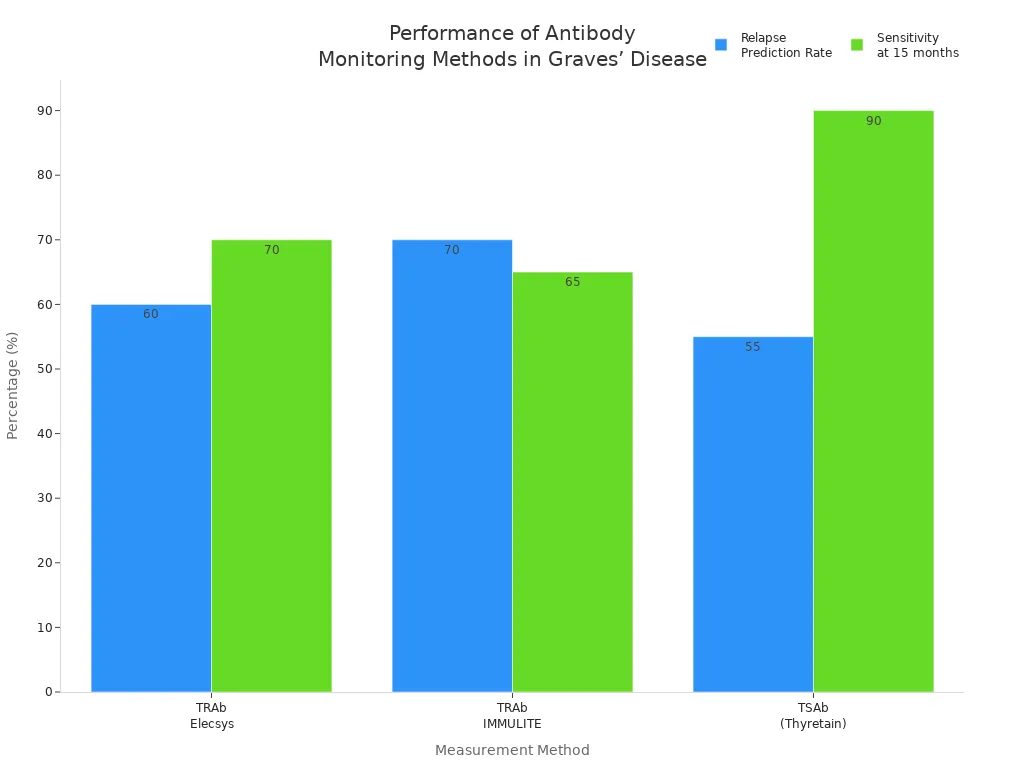
Treatment Implications
Your antibody status helps your doctor choose the best treatment for you. The table below shows how thyrotropin receptor antibodies affect decisions:
| Role of TSHR-Ab in Graves’ Disease Management | Description |
|---|---|
| Diagnostic Value | TSHR-Ab serves as a marker for diagnosing hyperthyroid Graves’ disease. |
| Severity Marker | The level of TSHR-Ab indicates the severity of the disease. |
| Influence on Therapy Choices | High levels of TSHR-Ab can guide the choice of treatment options such as antithyroid drugs, radioiodine treatment, or surgery. |
You may start with antithyroid drugs, which are safe and work well. Some people need radioactive iodine therapy or surgery. Beta-blockers help with symptoms but do not change your thyroid function. If your thyrotropin receptor antibody levels stay high, you may need longer treatment. Doctors sometimes keep you on antithyroid drugs for more than 24 months to help you reach remission and lower your risk of relapse. You see how important these antibodies are for diagnostic and management purposes.
You now know why TSH receptor autoantibodies matter for your thyroid health. These antibodies help doctors diagnose Graves’ disease, guide treatment, and predict outcomes.
- New research shows that measuring these antibodies can reveal if you are at risk for hyperthyroidism or hypothyroidism.
- Treatments like K1‐70TM can change thyroid function and improve eye symptoms.
- The American Thyroid Association and Clinical Thyroidology for the Public offer updates on thyroid research.
| Antibody Type | What It Means for You |
|---|---|
| Thyrotropin receptor antibody | Key sign of Graves’ disease |
| Antibody testing | Guides your treatment choices |
Stay curious and talk to your doctor if you have thyroid concerns. Staying informed helps you take charge of your health.
FAQ
What symptoms suggest I should get tested for TSH receptor autoantibodies?
You may notice weight changes, fast heartbeat, anxiety, or eye problems. These signs often point to thyroid issues. If you see these symptoms, ask your doctor about testing for TSH receptor autoantibodies.
Can TSH receptor autoantibodies go away on their own?
These antibodies often stay in your blood for years. Some people see levels drop after treatment. Regular checkups help you and your doctor track changes over time.
Do children with Graves’ disease need different tests than adults?
Doctors use the same blood tests for children and adults. The TRAb test works well for both groups. Early testing helps children get the right care quickly.
How do TSH receptor autoantibodies affect pregnancy?
High levels can cause problems for you and your baby. Your doctor may check your antibody levels if you have Graves’ disease and plan to become pregnant.
Can lifestyle changes lower TSH receptor autoantibody levels?
Healthy habits support your thyroid, but they do not remove these antibodies. You still need medical treatment. Always follow your doctor’s advice for the best results.